

Physiology and consequences of lung hyperinflation in COPD
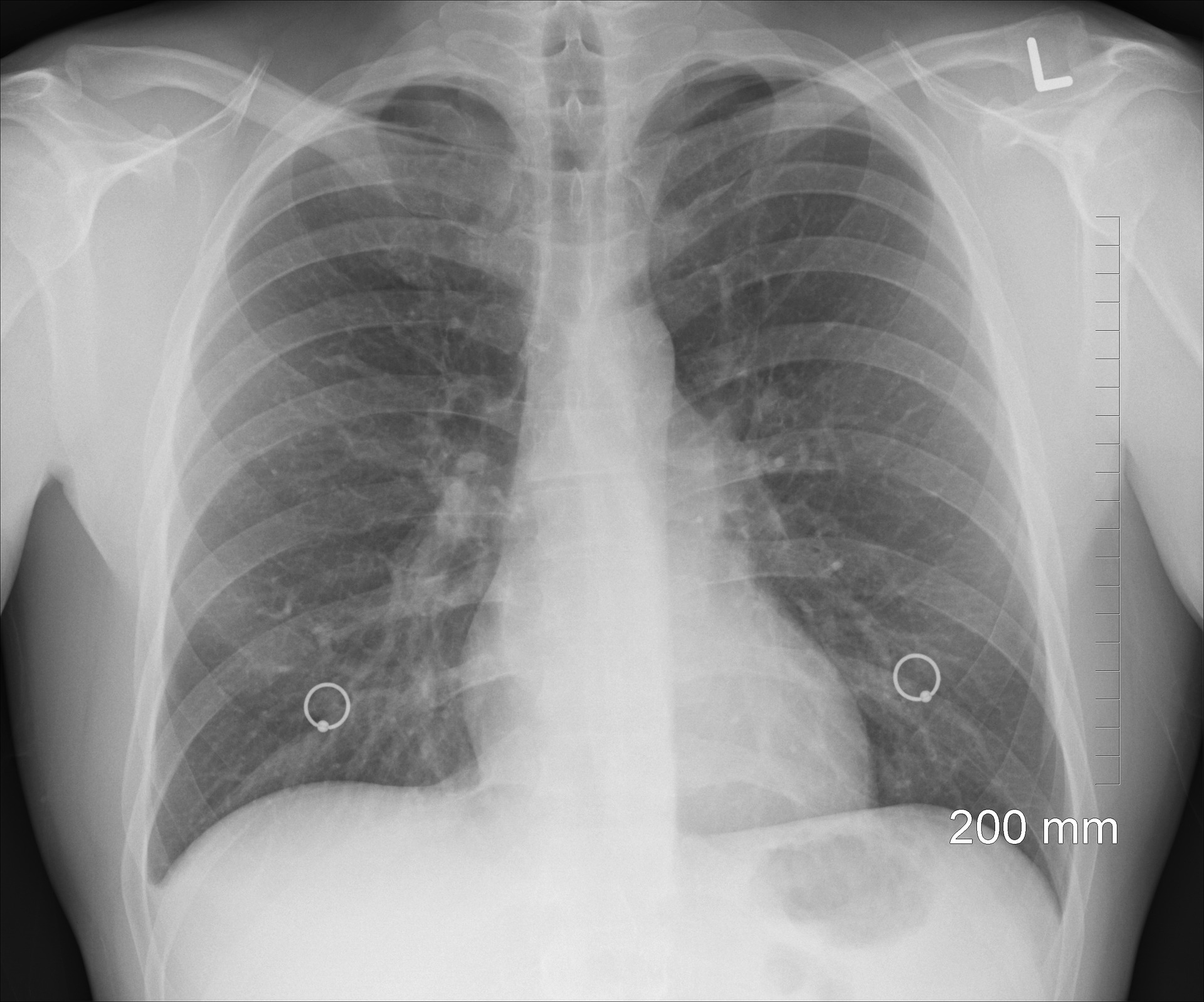
Hyperinflated lungs occur when air gets trapped in the lungs and reasons them to overinflate. Hyperinflated lungs may be because of blockages in the air passages or through air sacs which are much less elastic, which interferes with the expulsion of air from the lungs. Lung hyperinflation is seen in COPD patients— a disease that consists of emphysema. Certain lung problems, along with asthma and cystic fibrosis, can also reason hyperinflation. In a few cases, lungs can seem hyperinflated on X-rays for motives unrelated to lung characteristics.
Chronic obstructive pulmonary disease (COPD) is characterized by poorly reversible airflow obstacles. The pathological hallmarks of COPD are irritation of the peripheral airlines and destruction of lung parenchyma or emphysema. The practical results of those abnormalities are expiratory airflow limitation and dynamic lung hyperinflation, which then increase the elastic load of the respiration device and reduce the overall performance of the respiration muscles. These pathophysiologic capabilities contribute notably to the improvement of dyspnea, workout intolerance, and ventilatory failure. Several remedies can also additionally palliate flow limitation, together with interventions that regulate the respiratory pattern (deeper, slower) along with pursed-lip breathing, workout training, oxygen, and a few drugs. Other healing procedures are aimed toward its amelioration, along with bronchodilators, lung volume reduction surgical treatment, or breathing mixtures of helium and oxygen. Finally, a few interventions, along with inspiratory stress support, alleviate the threshold load related to flow limitation. The degree of flow limitation may be assessed through sure spirometry indexes, along with essential potential and inspiratory potential, or through different greater complexes indexes along with residual quantity/overall lung potential or practical residual potential/overall lung potential.
Two of the best methods to measure flow obstacles are to superimpose a flow-volume loop of a tidal breath inside a most flow-volume curve or to apply a negative expiratory stress technique. Likely this approach is greater correct and may be used at some stage in spontaneous respiration. A definitive definition of dynamic lung hyperinflation is missing in the literature, however, serial measurements of inspiratory potential at some stage in exercise will record the fashion of end-expiratory lung volume and allow setting up relationships with other measurements along with dyspnea, respiratory pattern, exercise tolerance, and gas exchange. Lung hyperinflation is seen in COPD.











